재발성 중이염(재발성 급성 중이염), Recurrent (acute) otitis media 1/27/2022
- 급성 중이염을 적절한 항생제로 적절히 기간 동안 치료해서 다 나은 후 불과 며칠이 지난 후나 몇 주가 지난 후 또다시 급성 중이염이 생기고 또 그 급성 중이염을 적절히 치료받았는데도 급성 중이염이 또다시 여러 번 재발될 때 재발성 중이염이라고 한다.
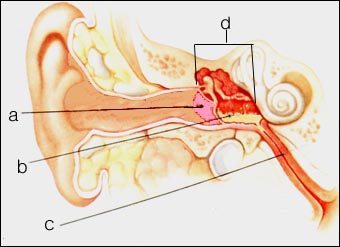
그림 55. 급성 중이염.
노란색으로 표시된 부분은 고름
a-고막, b-고름, c-이관, d-중이.
Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
재발성 중이염의 원인
- 재발성 중이염을 일으키는 박테리아는 급성 중이염을 일으키는 박테리아와 거의 같다.
- 폐렴연쇄상구균이나 헤모필러스인플루엔자균, 부란햄엘라카탈라리스균, 또는 A군 베타 용혈성 연쇄상구균 등이 재발성 중이염의 주 원인 세균이다.
- 급성 중이염을 적절히 치료받고 다 나은 후 또 급성중이염이 재발되는 이유를 확실히 모를 때도 많다.
- 기관지 천식, 알레르기성 비염, 또는 아토피성 피부염 등을 현재 앓고 있거나 과거에 앓았던 병력이 있는 아이들이나 아토피성 체질이 있는 아이들은 급성 중이염에 더 잘 걸릴 수 있고, 또 그들에게 재발성 중이염, 또 삼출성 중이염이 더 잘 생길 수 있다.
- 감기나 다른 종류의 바이러스성 상·하기도 염이 많이 유행되는 겨울철에 바이러스성 상·하기도염 등을 앓을 때마다 이차 세균 감염이 중이 강 속에 생겨 급성 중이염에 걸릴 수 있고 재발성 중이염에 더 잘 걸릴 수 있다.
- 급성 중이염을 적절한 항생제로 적절히 치료해서 중이염을 일으킨 중이강 내 박테리아가 다 죽은 후 얼마동안 중이강 속에 삼출액이 계속 남아 있을 수 있다.
- 연구에 의하면, 항생제로 급성 중이염을 적절히 치료하기 시작한 첫 날 부터 14~90일까지 삼출액이 중이 강 속에 계속 괴어 있을 수 있다.
- 급성 중이염을 적절한 기간 동안 항생제로 적절히 치료하여 그 중이염을 일으킨 박테리아가 다 죽은 후에도 중이 강 속에 괴어 있는 삼출액은 세균이 자라는데 좋은 영양 배지가 될 수 있다.
- 또 다른 어떤 박테리아가 그 삼출액이 있는 중이 강 속에 감염될 때 박테리아는 더 쉽게 자랄 수
- 있고 결국 재발성 중이염이 쉽게 생기게 된다.
- 급성 중이염의 30%는 적절히 치료한 후부터 30일까지 세균이 없는 삼출액이 중이 강 속에 계속 남아 있을 수 있다.
- 또 같은 연구에 의하면, 적절히 치료한 급성 중이염의 10%는 적절히 치료를 마친 후 90일까지 세균이 없는 삼출액이 중이 강 속에 계속 남아 있을 수 있다.
- 이와 같이 급성 중이염을 적절히 치료해서 완전히 회복되는 동안에도 세균이 없는 삼출액이 중이 강 속에 계속 오랫동안 남아 있을 수 있다.
- 급성 중이염이 완전히 회복되는 과정 동안 감기나 알레르기성 비염, 또는 바이러스성 상·하기도염 등에 걸리면 이관이 막히고 박테리아가 중이 강 삼출액에 또 다시 감염되면 급성 중이염이 또 다시 생기게 된다.
- 이런 식으로 급성 중이염이 생기고 그것이 잘 치료되면 완전히 나을 수도 있고 또 완전히 나아가는 중 세균에 감염되어 또 다시 급성 중이염이 재발되어 재발성 중이염이 생기게 된다. 알레르기성 비염 참조.
Update 5/13/2021 The NEJM
2921년 5월 13일 업데이트 NEJM
재발성 급성 중이염은 소아에게 항생제 치료를 요하는 가장 흔한 감염병 중 하나이다.
이 병은 주로 감기등 상기도 바이러스 감염으로 생기는 유스타키오관 기능 장애에 기인하며, 유병률은 6개월에서 12개월 사이의 소아에서 가장 많이 생긴다. 12개월 미만 아이들은 은 재발성 급성 중이염의 발병에 취약하다. 이는 6개월 이내에 급성 중이염이 3회 이상 발생하거나 12개월 이내에 4회 이상 발생하면재발성 급성 중이염이러고 한다.
Acute otitis media is one of the most common indications for both seeking medical care and prescribing antibiotics for children. The disorder is attributable to eustachian-tube dysfunction, which is most often caused by viral upper respiratory infections, and its prevalence is highest in children between 6 and 12 months of age2 Young children who have the first episode of acute otitis media early in life (<12 months) are susceptible to the development of recurrent acute otitis media — defined as the occurrence of at least three episodes of acute otitis media within 6 months or four episodes within 12 months.
재발성 중이염의 증상 징후
- 급성 중이염의 증상 징후와 거의 비슷하다.
- 아토피성 체질이 있는 아이들이나 아토피성 피부염이나 알레르기성 비염, 또는 기관지 천식 등의 알레르기성 질환의 병력이 있는 아이들은 재발성 중이염에 더 잘 걸린다.
- 재발성 중이염의 증상 징후는 재발성 중이염에 잘 걸리게 하는 상·하기도 염 또는 감기나 알레르기성 질환 등의 증상 징후가 함께 있는 것이 보통이다 .
재발성 중이염의 진단
- 병력, 증상 징후와 진찰소견 등을 종합하여 이병이 의심되면 이경으로 외이도 속을 통해 고막을 진찰해서 쉽게 진단할 수 있다.
- 아토피성 체질이 있는 아이들, 아토피성 피부염이나 기관지 천식, 또는 알레르기성 비염 등의 병력이 있는 아이들은 재발성 중이염에 더 잘 걸리기 때문에 그런 병력이 있으면 진단하는 데 큰 도움이 된다.
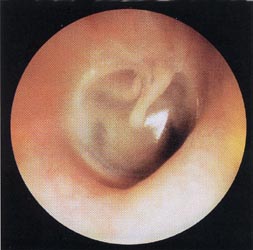
사진 56. 이경으로 외이도 속을 통해 육안으로 본 정상 고막.
출처- Otitis media, Roche laboratories
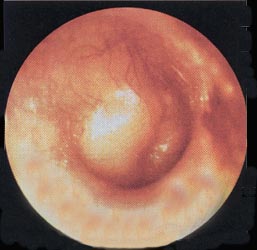
사진 57. 급성 중이염이 있을 때 이경으로 외이도 속을 통해 육안으로 본 고막.
고막이 팽창 되어 있고 발적되어 있다.
출처- Otitis Media, Roche laboratories
재발성 중이염의 치료
- 급성 중이염을 치료할 때와 같이 적절한 항생제로 치료한다.
- 드물게 중이 강 속에 괸 고름을 주사 바늘로 빼 그 고름 피검 물로 그람 염색 세균 현미경 검사와 세균배양검사와 항생제 감수성검사를 해서 그 결과에 따라 적절한 항생제를 선택해 치료할 수 있다.
- 고막을 째고 중이 속에 괴어 있는 고름을 빼고 경구용 항생제 투여로 치료할 수도 있다.
- 급성 중이염이 자주 재발될 때는 외이도 속과 중이 강 사이에 공기가 잘 유통되게 고막에 조그마한 통기관 삽입수술을 해 치료한다.
- 이런 통기관 삽입수술 치료로 재발성 중이염을 치료할 때 난청, 고막, 출혈, 또는 고막천공 등 부작용이 생길 수 있다.
- 이런 수술치료는 최종 선택 치료방법이다.
- 재발성 급성 중이염을 적절한 항생제로 적절한 기간 동안 치료한 후 중이염이 완치됐는지 확인하기 위해 의사의 추후 재 검진을 꼭 받아야 한다.
- 적절한 항생제로 몇 개월 동안 만성 재발성 중이염을 예방적 치료를 하기도 한다.
Recurrent otitis media
• Recurrence when acute otitis media develops again only a few days or weeks after the acute otitis media has been properly treated with appropriate antibiotics for a period of time, and the acute otitis media recurs several times even though the acute otitis media has been properly treated. It is called otitis media.
Figure 55. Acute otitis media. The area marked in yellow is pus a – tympanic membrane, b – pus, c – ear canal, d – middle ear. Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
Causes of recurrent otitis media
• The bacteria that cause recurrent otitis media are almost the same as those that cause acute otitis media.
• Streptococcus pneumoniae, Haemophilus influenzae, Branham ella catalaris, or group A beta-hemolytic streptococcus are the main causes of recurrent otitis media.
• In many cases, it is not clear why acute otitis media recurs after being properly treated and cured.
• Children with a current or past history of bronchial asthma, allergic rhinitis, or atopic dermatitis, or children with atopic constitution, are more likely to develop acute otitis media, and they Otitis media with effusion may be more likely.
• In winter, when colds and other types of viral upper and lower respiratory tract infections are prevalent, whenever you suffer from viral upper and lower respiratory tract infections, a secondary bacterial infection occurs in the middle ear cavity, which can lead to acute otitis media and make you more susceptible to recurrent otitis media. can
• When acute otitis media is properly treated with appropriate antibiotics, exudate may remain in the middle ear cavity for some time after the bacteria in the middle ear cavity that caused the otitis media are killed.
• Studies have shown that effusion can remain in the middle ear cavity from the first day of adequate antibiotic treatment for acute otitis media to 14 to 90 days.
• Even after acute otitis media is properly treated with antibiotics for an appropriate period and the bacteria causing the otitis media are dead, the exudate remaining in the middle ear cavity can be a good nutrient medium for bacteria to grow.
• When another bacteria infects the middle ear cavity with the exudate, the bacteria can grow more easily. • and eventually recurrent otitis media easily develops.
• In 30% of acute otitis media, bacteria-free exudate may remain in the middle ear cavity for up to 30 days after adequate treatment.
• Another study found that in 10% of properly treated acute otitis media, bacteria-free effusion could remain in the middle ear cavity for up to 90 days after adequate treatment.
• Even during a full recovery with proper treatment of this acute otitis media, bacteria-free exudate can remain in the middle ear cavity for a long time.
• If you catch a cold, allergic rhinitis, or viral upper and lower respiratory tract while the acute otitis media is fully recovered, the ear canal is blocked, and if the bacteria are re-infected with the middle ear cavity effusion, acute otitis media will occur again.
• In this way, if acute otitis media occurs and it is treated well, it may be completely cured, or if it is fully treated, it may become infected with bacteria and cause acute otitis media to recur, resulting in recurrent otitis media. See Allergic Rhinitis.
Symptoms, signs of recurrent otitis media
• Symptoms are similar to those of acute otitis media.
• Children with the atopic constitution or with a history of allergic diseases such as atopic dermatitis, allergic rhinitis, or bronchial asthma are more likely to develop recurrent otitis media.
• Symptomatic signs of recurrent otitis media usually include symptoms such as upper and lower respiratory tract infections that predispose to recurrent otitis media, colds, or allergic diseases.
Diagnosis of recurrent otitis media
• If the otitis is suspected by synthesizing the medical history, symptom signs, and examination findings, it can be easily diagnosed by examining the tympanic membrane through the inside of the external auditory canal with an otoscope.
• Children with the atopic constitution, children with a history of atopic dermatitis, bronchial asthma, or allergic rhinitis are more prone to recurrent otitis media, so having such a history is of great help in the diagnosis.
Photo 56. Normal tympanic membrane seen with the naked eye through the auditory canal. Source- Otitis media, Roche laboratories
Photo 57. The tympanic membrane as seen through the inside of the external auditory meatus through the otoscope in acute otitis media. The eardrum is inflamed and reddened. Source- Otitis Media, Roche laboratories
Treatment of recurrent otitis media
• Treat with appropriate antibiotics as in the treatment of acute otitis media.
• Rarely, pus from the middle ear cavity is removed with a needle and the pus sample is used for Gram-stained microscopic examination, bacterial culture, and antibiotic susceptibility test, and the appropriate antibiotic can be selected and treated according to the results.
• It can be treated with an oral antibiotic to remove the pus from the middle ear by cutting the eardrum.
• When acute otitis media frequently recurs, it is treated by inserting a small ventilation tube into the eardrum so that air can circulate well between the inner ear canal and the middle ear cavity.
• Side effects such as hearing loss, eardrum, hemorrhage, or perforation of the eardrum may occur when treating recurrent otitis media with such ventilator implantation treatment.
• This type of surgical treatment is the final treatment option.
• After treating recurrent acute otitis media with appropriate antibiotics for an appropriate period of time, it is essential to undergo a follow-up examination by a doctor to confirm that the otitis media has been cured.
• Prophylactic treatment of chronic recurrent otitis media for several months with appropriate antibiotics.
Update 5/13/2021 The NEJM
2921년 5월 13일 업데이트 NEJM
재발성 급성 중이염은 소아에게 항생제 치료를 요하는 가장 흔한 감염병 중 하나이다.
이 병은 주로 감기등 상기도 바이러스 감염으로 생기는 유스타키오관 기능 장애에 기인하며, 유병률은 6개월에서 12개월 사이의 소아에서 가장 많이 생긴다. 12개월 미만 아이들은 은 재발성 급성 중이염의 발병에 취약하다. 이는 6개월 이내에 급성 중이염이 3회 이상 발생하거나 12개월 이내에 4회 이상 발생하면재발성 급성 중이염이러고 한다.
Acute otitis media is one of the most common indications for both seeking medical care and prescribing antibiotics for children. The disorder is attributable to eustachian-tube dysfunction, which is most often caused by viral upper respiratory infections, and its prevalence is highest in children between 6 and 12 months of age2 Young children who have a first episode of acute otitis media early in life (<12 months) are susceptible to the development of recurrent acute otitis media — defined as the occurrence of at least three episodes of acute otitis media within 6 months or four episodes within 12 months.
출처 및 참조 문헌
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
-
제18권 소아청소년 이비인후과 질환 참조문헌 및 출처
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Gray’s Anatomy
-
Habilitation of The handicapped Child, The Pediatric Clinics of North America, Robert H Haslam, MD.,
-
Pediatric Otolaryngology Sylvan Stool
-
Hearing Loss In children, The Pediatric Clinics of North America Nancy Roizen,MD and Allan O Diefendorf, PhD
-
Recent Advances in Pediatric otolaryngology The Pediatric Clinics of North America
-
Pediatric Otolaryngology. The Pediatric Clinics of North America, David Tunkel, MD., Kenneth MD Grundfast, MD
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.